
臨床實務改變差異:ATA 2015 vs 2025 DTC Guidelines
日期: 2026-03-10 | 版本: v1.4
目錄索引(Table of Contents)
- 本文件閱讀指引
- 1. Lobectomy 適用範圍擴大至 ≤2 cm 為強力預設
- 2. 低風險 DTC 的 RAI:Strong/High Evidence 反對使用
- 3. 預防性 CND:「Strong 推薦不做」(非 Conditional)
- 4. 術後風險分層:3 級 → 4 級系統(RAI 和 TSH 決策精細化)
- 5. TSH 抑制動態化:靜態 Initial Risk → Dynamic Response-to-Therapy
- 6. 監測終點定義:5–8 年 US,10–15 年「Complete Remission」
- 7. Active Surveillance 正式獲得背書(從 2015 R12 提升)
- 8. cT2(2–4 cm)的 Lobectomy:Conditional Preference(確定性較低)
- 9. RAI-Refractory DTC 的 Precision Oncology(突變特異性靶向治療)
- 10. Completion Thyroidectomy 降級(Conditional 取代 Strong)
- 11. Shared Decision-Making (SDM) 形式化
- 12. De-escalation Narrative Analysis(去強化敘事分析)
本文件閱讀指引
每項變更包含以下面向:
- 變更內容(What Changed) — 精確的 recommendation 原文與引用
- 變更原因(Why It Changed) — guideline 所引據的 evidence 與 rationale
- 關鍵文獻(Key References) — 直接整合文獻分析(含 PMID、研究設計、數據)
- 影響族群(Who Is Affected) — 受影響的特定患者群體
- 臨床實務調整(What to Do Differently) — 具體的週一早上可執行事項
- 注記 — 重要的精確性說明
1. Lobectomy 適用範圍擴大至 ≤2 cm 為強力預設
變更概述
2015 guideline 將 lobectomy 的默認適用範圍限於 <1 cm 的 cN0 intrathyroidal PTC(R35C),1-4 cm 腫瘤列為 lobectomy 與 total thyroidectomy 均可之選項(R35B)。2025 guideline 將 lobectomy 的默認適用上限擴大至 <=2 cm(R15A, Strong/Moderate),且對 2-4 cm 腫瘤首次以 lobectomy 為「preferred」選項(R15B, Conditional/Low-moderate)。
變更內容
| 2015 | 2025 | |
|---|---|---|
| Recommendation | R35C: 腫瘤 <1 cm、cN0、無 ETE 者行 lobectomy | R15A: 腫瘤 ≤2 cm(cT1N0M0)者「should be」lobectomy |
| Strength | Strong recommendation, Moderate-quality evidence | Strong recommendation, Moderate certainty evidence |
| 大小閾值 | <1 cm | ≤2 cm |
Strong lobectomy 預設的適用腫瘤大小範圍增加了一倍。1–2 cm 腫瘤在 2015 年屬臨床均勢區(R35B:「can be either」),現已納入 strong lobectomy recommendation。
變更原因
2025 guideline(R15 討論,p.861–862)提供明確 rationale:
- 多項大型 registry 研究和傾向評分配對研究在校正 confounders 後,顯示 ≤2 cm PTC 的 lobectomy 與 total thyroidectomy 存活率無差異。
- Total thyroidectomy 併發症率約為 lobectomy 的 2 倍(高量外科醫師 OR=1.82,Hauch 2014)。
- ESTIMABL2 和 IoN Trial 消除了對 total thyroidectomy 的主要歷史理由(以利 RAI 治療)。
- AJCC 8th 版將 microscopic ETE 移出 T3 分期,使大量患者降期。
關鍵文獻
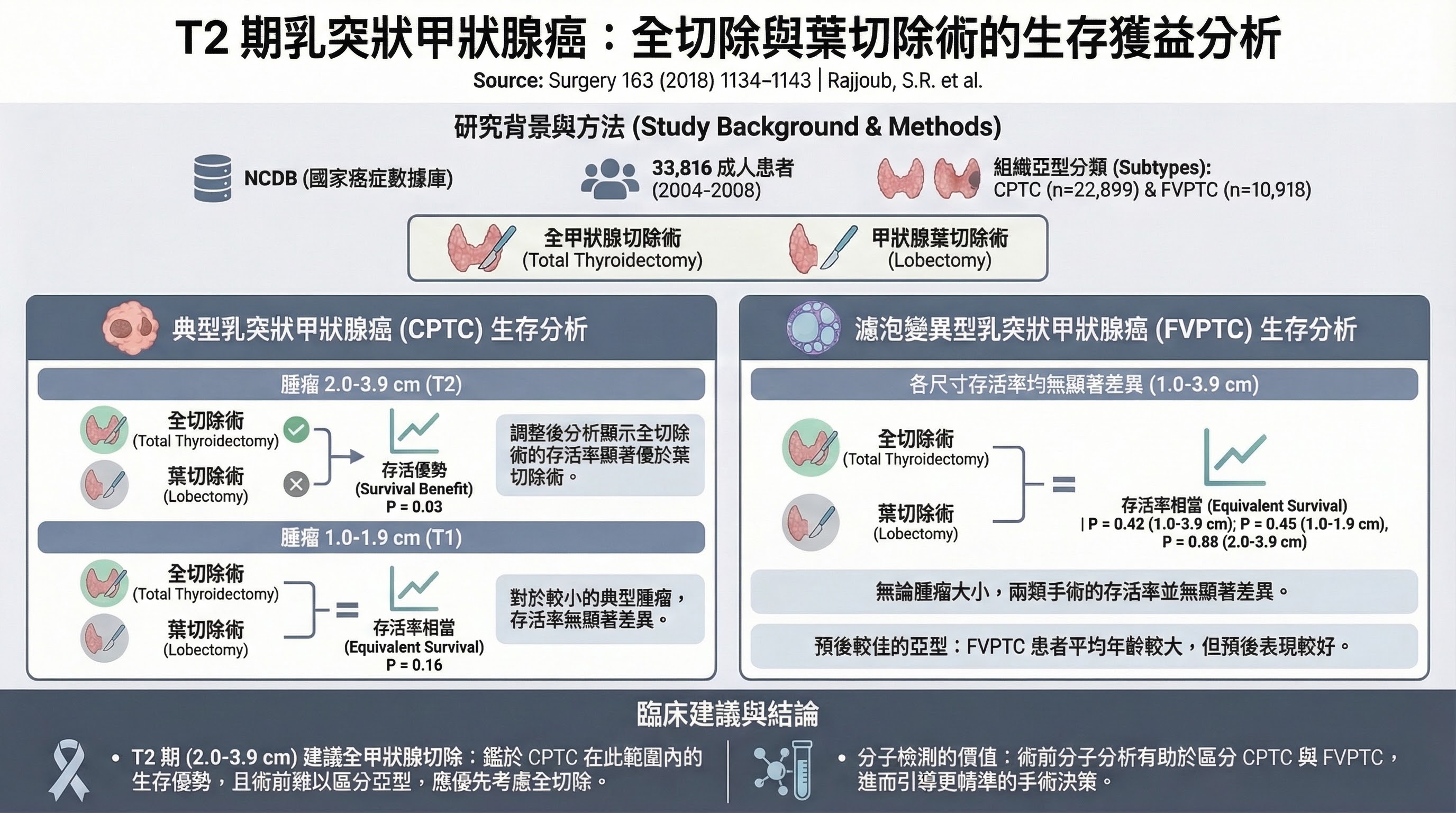
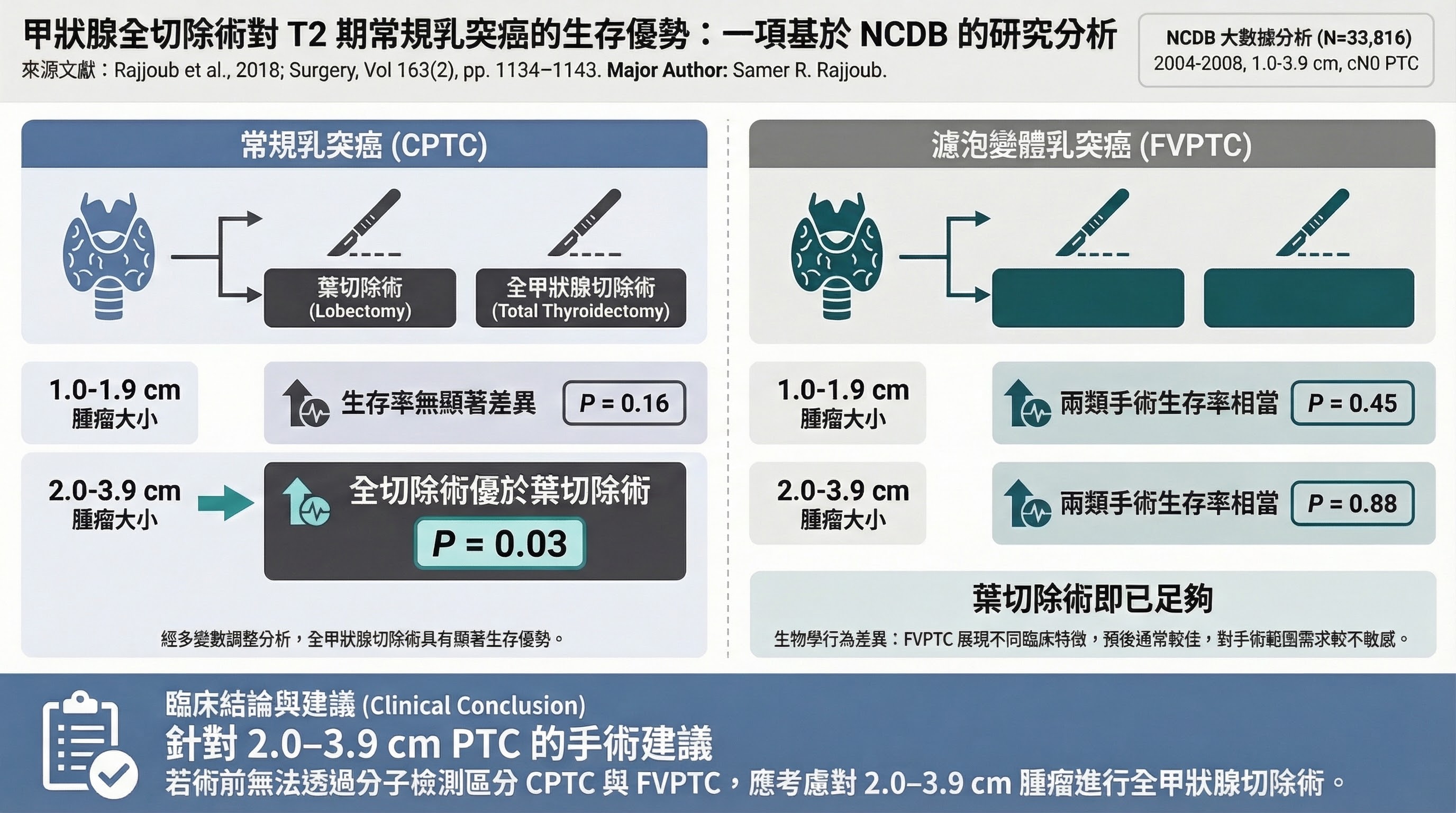
■ 關鍵文獻:Rajjoub et al. 2018(PMID: 29426618)
- Citation: Rajjoub SR et al., Surgery 2018;163(6):1134–1143
- 研究設計: 回溯性 NCDB cohort,N=33,816(1–3.9 cm PTC,cN0,2004–2008)
- PICO: P=1–3.9 cm PTC cN0, I=total thyroidectomy, C=lobectomy, O=overall survival(中位追蹤 6.49 年)
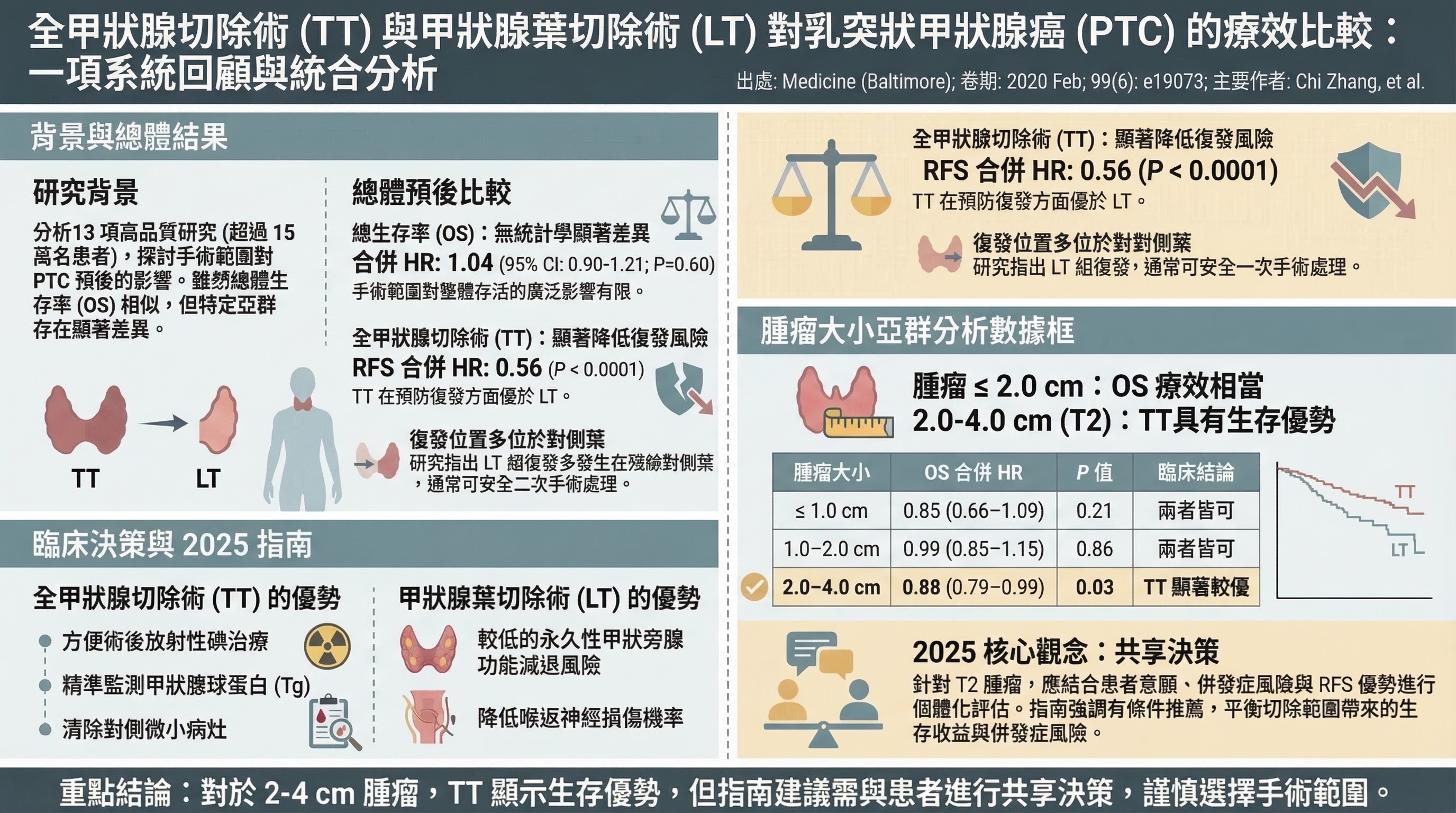
- 主要發現: CPTC 1.0–1.9 cm:lobectomy HR 0.76(95% CI 0.51–1.12, P=0.1596)— 無差異;CPTC 2.0–3.9 cm:lobectomy HR 1.53(95% CI 1.06–2.19, P=0.0226)— TT 有邊際優勢;FVPTC 所有大小均無差異(P>0.4)
- 為什麼支持此 recommendation 變更: 對 ≤2 cm PTC 顯示 lobectomy 無存活差異(支持 R15A),對 2–4 cm CPTC 顯示 TT 有邊際優勢(解釋 R15B 為何為 Conditional)
- 主要限制: 回溯性;NCDB 缺乏 Tg 和 RAI 完整記錄;2004–2008 年代幾乎所有 TT 患者均接受 RAI
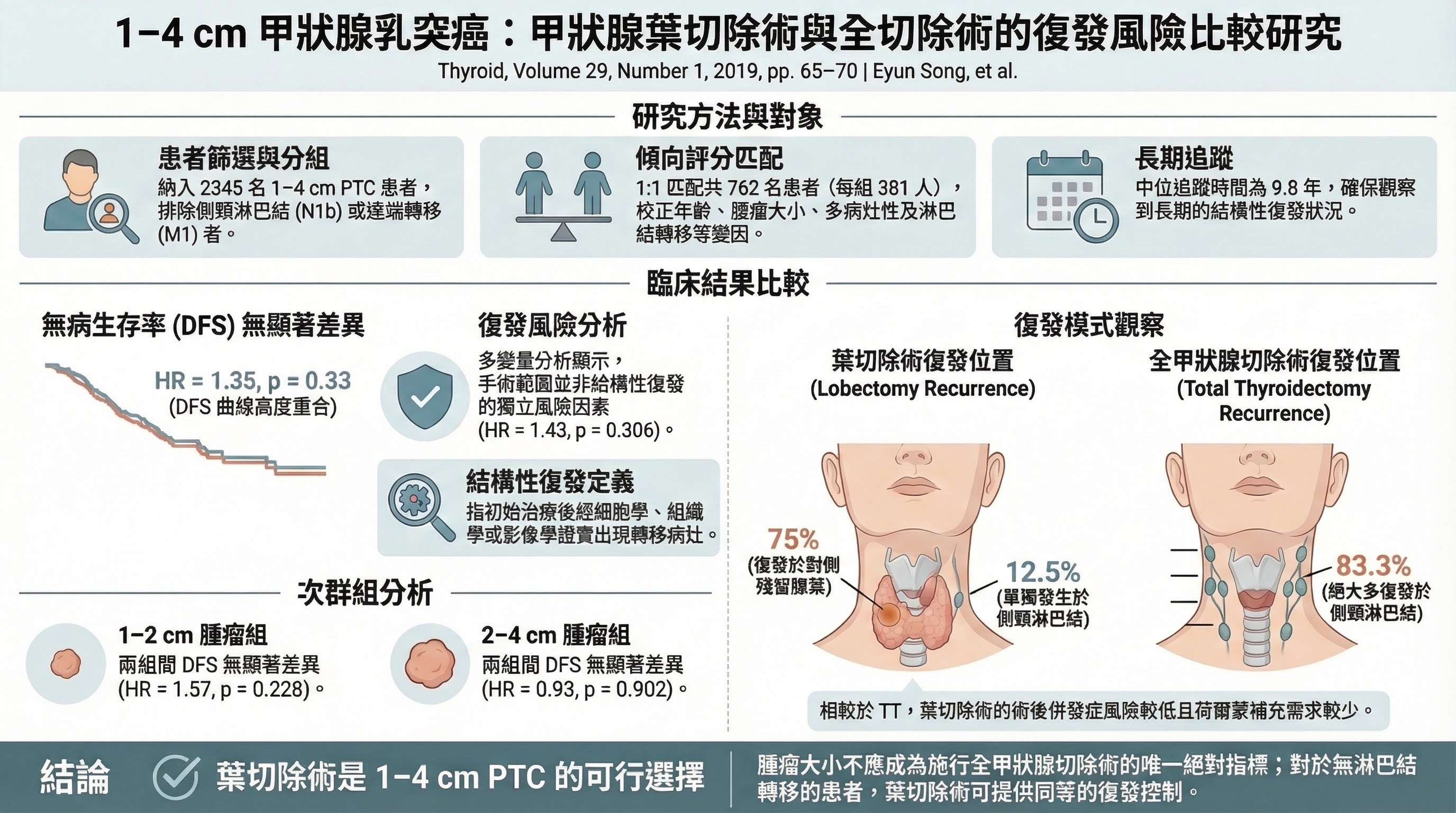
■ 關鍵文獻:Song et al. 2019(PMID: 30375260)
- Citation: Song E et al., Thyroid 2019;29(1):64–70
- 研究設計: 單中心回溯性傾向評分配對研究,N=2,345 PTC(1–4 cm),配對後各組 381 例
- PICO: P=1–4 cm PTC cN0, I=lobectomy, C=total thyroidectomy, O=disease-free survival(structural persistent/recurrent disease)
- 主要發現: 中位追蹤 9.8 年;配對後 DFS:HR=1.35(CI 0.79–2.28, P=0.33)無差異;1–2 cm 亞組 HR=1.57(CI 0.75–3.25, P=0.228);2–4 cm 亞組 HR=0.93(CI 0.30–2.89, P=0.902)
- 為什麼支持此 recommendation 變更: 長達近 10 年追蹤確認 1–4 cm PTC 的 DFS 在 lobectomy 和 TT 之間無差異,直接支持 R15A 的強推薦
- 主要限制: 單一亞洲中心;TT 組幾乎全部接受 RAI(93.9%),lobectomy 組無 RAI;所有患者均常規接受 prophylactic CCND
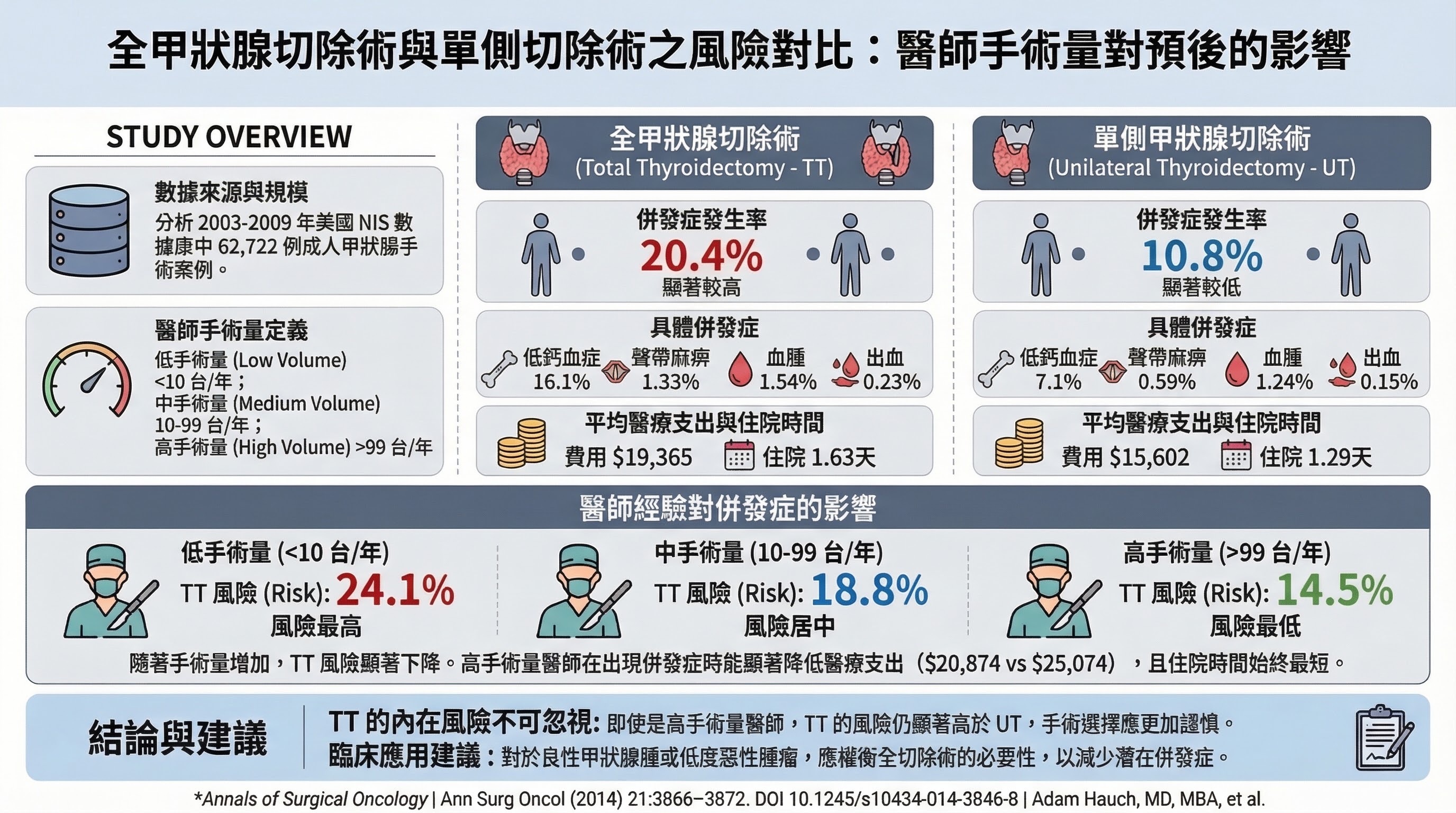
■ 關鍵文獻:Hauch et al. 2014(PMID: 24943236)
- Citation: Hauch A et al., Ann Surg Oncol 2014;21(13):4236–4242
- 研究設計: 橫斷面研究(Nationwide Inpatient Sample 2003–2009),N=62,722 例
- 主要發現: 整體併發症率:TT 20.4% vs UT 10.8%;調整後 OR=2.154(CI 1.987–2.334)。高量外科醫師(>99 cases/yr):TT 14.5% vs UT 7.6%,調整後 OR=1.824(CI 1.458–2.281)——說明高手術量無法消除 TT 相對於 UT 的結構性風險差異
- 為什麼支持此 recommendation 變更: 即使是最有經驗的外科醫師,TT 風險仍為 lobectomy 的 1.82 倍,為 lobectomy 優先提供強有力的 morbidity 依據
- 主要限制: 橫斷面設計;ICD-9 碼;良惡性混合;無長期腫瘤學結果
影響族群
具有單側、intrathyroidal DTC 介於 1–2 cm(cT1bN0M0)的患者。估計佔新診斷 PTC 的 40–50%。
臨床實務調整
- 外科醫師: 所有 cT1N0M0 DTC(至 2 cm)預設行 lobectomy;total thyroidectomy 保留給 bilateral disease、prior radiation、familial DTC 或患者偏好
- Tumor board: 對 1–2 cm cN0 DTC 倡議 lobectomy;在此大小範圍行 total thyroidectomy 需有特定理由
- 患者諮詢: 說明 lobectomy 的手術風險約為 total thyroidectomy 的一半;70–80% 的 lobectomy 患者可完全保留甲狀腺功能;約 10–15% 可能需要 completion thyroidectomy
- 下游影響: Lobectomy 患者不進入 RAI 決策流程,也不需要 TSH 抑制或終身 thyroid hormone replacement
連結到具體 Recommendation 變更
此深層理據直接解釋了以下 recommendation 變更:
- R15A(<=2 cm 默認 lobectomy)← registry 數據 + 併發症量化
- R15B(2-4 cm lobectomy preferred)← 同上 + SDM + 矛盾證據
- R16(completion thyroidectomy 從 "should be offered" 降為 "may be considered")← lobectomy 適用範圍擴大的邏輯延伸
- R6(surgeon volume 正式 recommendation)← 併發症率與手術量高度相關
注記
- 注意: bilateral multifocality 或具臨床意義的 contralateral nodularity(存在於 30–50% 患者)仍可能傾向 total thyroidectomy
- 複合效應: Lobectomy 擴展 + no RAI + no TSH suppression = 三重 de-escalation,但此組合路徑尚無前瞻性研究作為 combined pathway 驗證
2. 低風險 DTC 的 RAI:Strong/High Evidence 反對使用
變更概述
2015 guideline 以 Weak/Low 推薦低風險 DTC 不常規使用 RAI(R51A)。2025 guideline 將其升級為 Strong/High(R32A)——這是整個 guideline 中推薦等級變化幅度最大的單項變更。
變更內容
| 2015 | 2025 | |
|---|---|---|
| Recommendation | R51A: 不常規建議對 ATA low-risk 使用 RAI(Weak/Low);R51B: 不建議用於 unifocal microPTC(Strong/Moderate) | R32A: 不建議對 low-risk 使用 RAI(Strong/High certainty) |
| 關鍵進步 | 對更廣泛低風險 DTC 僅 Weak/Low | 升級幅度最大:Weak/Low → Strong/High(針對非 microPTC 低風險族群) |
注意: 對 unifocal microPTC 亞群,2015 R51B 已為 Strong/Moderate;升級幅度為 Strong/Moderate → Strong/High(較小幅度)。整份 guideline 中證據品質躍升最大的是針對更廣泛低風險 DTC 族群(R51A 適用人群)。
變更原因
ESTIMABL2 + IoN Trial 兩個 Phase 3 RCT 的收斂結果,使 High certainty evidence 的認定成為可能。
關鍵文獻
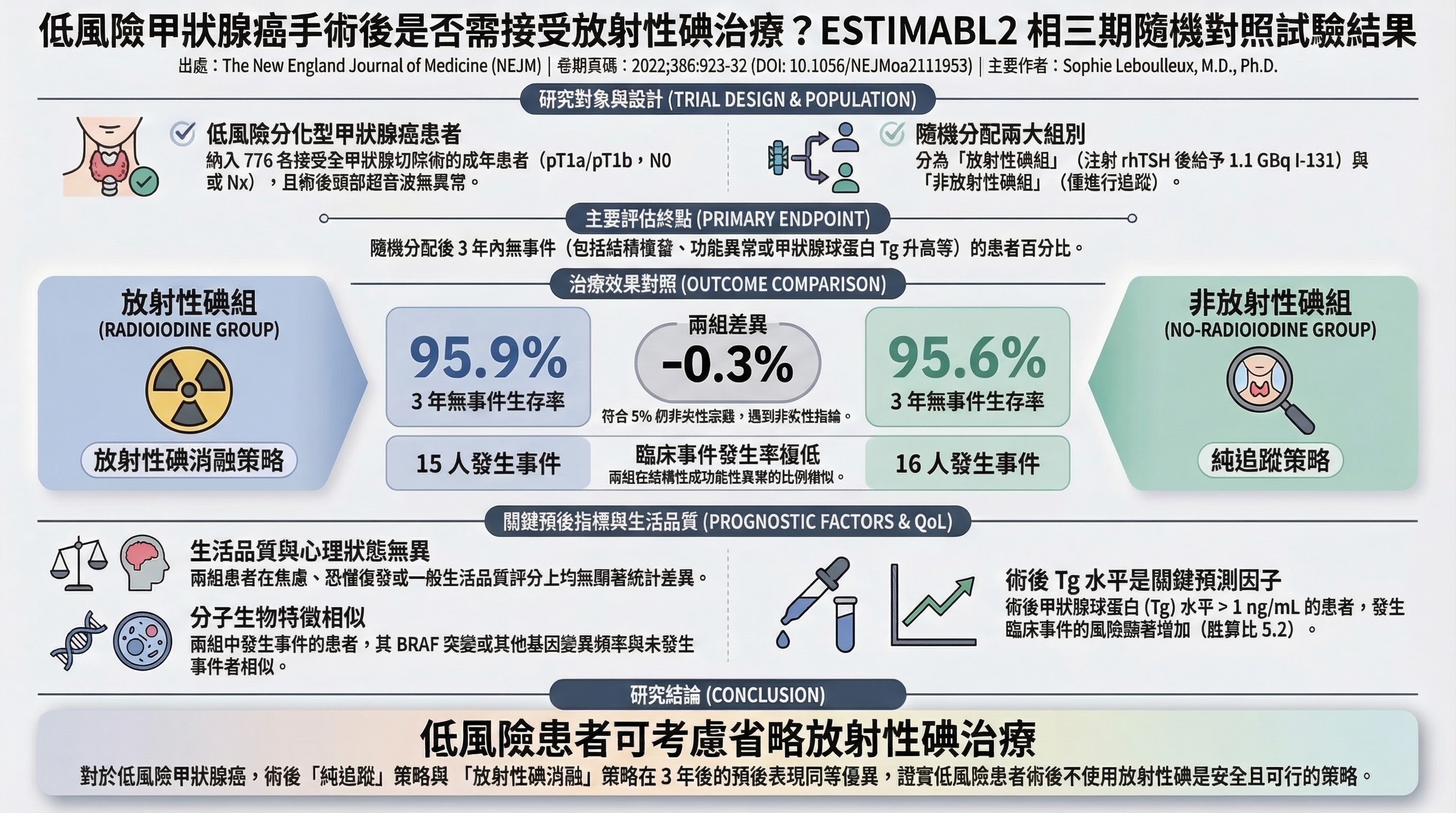
■ 關鍵文獻:ESTIMABL2 Primary(PMID: 35263518)
- Citation: Leboulleux S et al., N Engl J Med, 2022; 386(10):923–932
- 研究設計: Phase 3 non-inferiority RCT,N=730 evaluable(776 enrolled),35 個法國中心,2013–2017
- PICO: P=低風險 DTC(pT1am 或 pT1b,N0/Nx,無 ETE),接受 total thyroidectomy;I=術後無 RAI;C=1.1 GBq RAI(rhTSH 後);O=3 年無事件率,非劣效性界限 5%
- 主要發現: 3 年無事件率:No-RAI 95.6%(CI 93.0–97.5)vs RAI 95.9%(CI 93.3–97.7),差異 -0.3%(90% CI -2.7 to 2.2)→ 非劣效性達標
- 次要發現: 生活品質評分兩組相似;除 RAI 組 lacrimal discomfort 外無差異
- 為什麼支持此 recommendation 變更: 首個 Phase 3 RCT 直接證明低風險 DTC 省略 RAI 的安全性,填補 2015 guideline 指出的關鍵空白
- 主要限制: 3 年追蹤(此次報告)相對短;open-label;在 TT 背景下進行(不適用於 lobectomy);複合終點含生物學事件
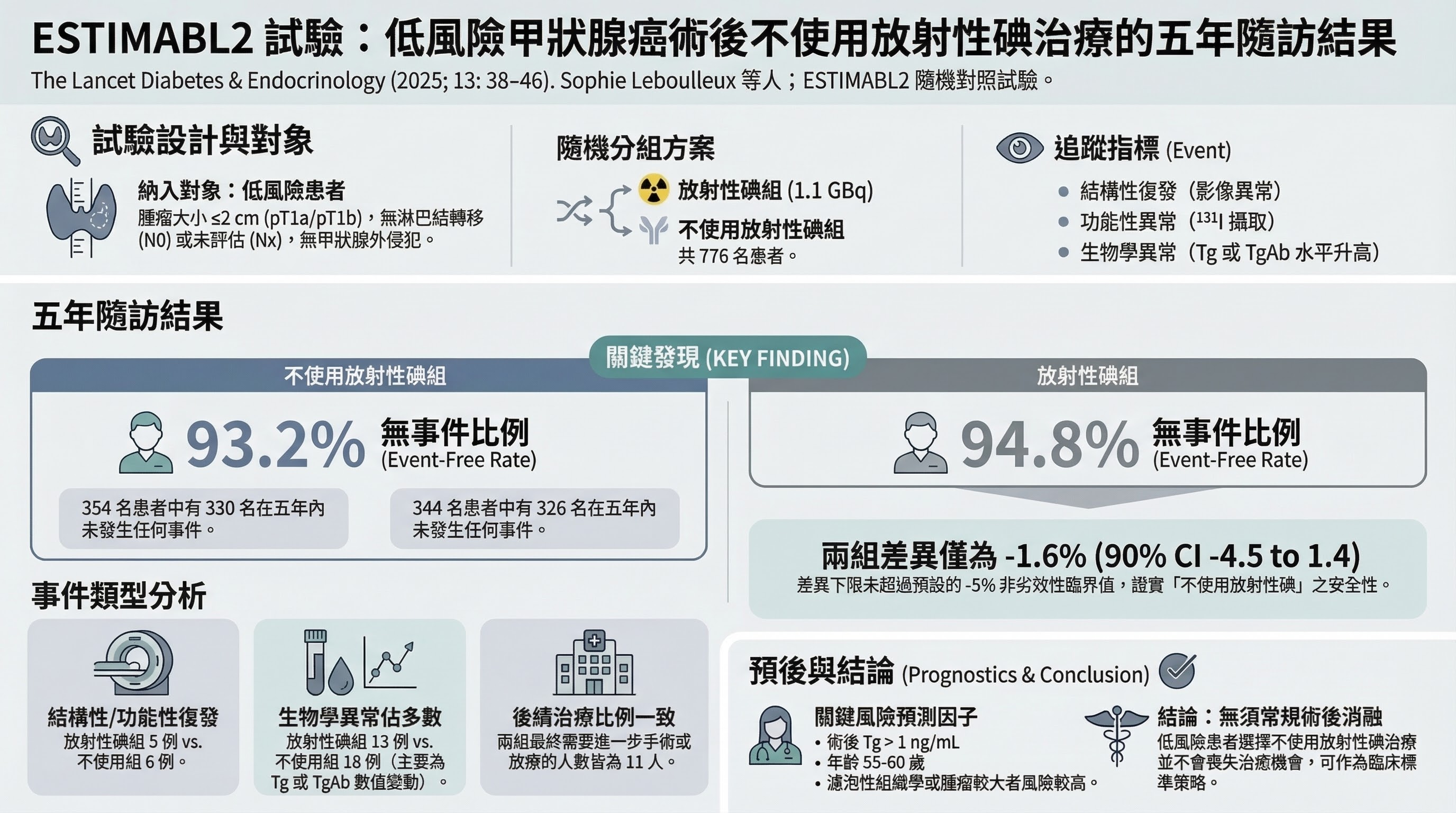
■ 關鍵文獻:ESTIMABL2 5-Year Follow-up(PMID: 39586309)
- Citation: Leboulleux S et al., Lancet Diabetes Endocrinol, 2025; 13(1):38–46
- 研究設計: Pre-specified secondary analysis,N=698 evaluable at 5 years
- 主要發現: 5 年無事件率:No-RAI 93.2%(CI 90.1–95.4)vs RAI 94.8%(CI 91.9–96.7),差異 -1.6%(90% CI -4.5 to 1.4)→ 非劣效性維持;5 年共 42 例事件(No-RAI 24 例,RAI 18 例)
- 為什麼支持此 recommendation 變更: 確認 5 年追蹤仍維持非劣效性,解決「3 年可能太短」的主要批評;2025 guideline R32 明確引用此 5 年資料
- 主要限制: 5 年仍可能尚短;No-RAI 組有略多的新增晚期事件;僅法國資料
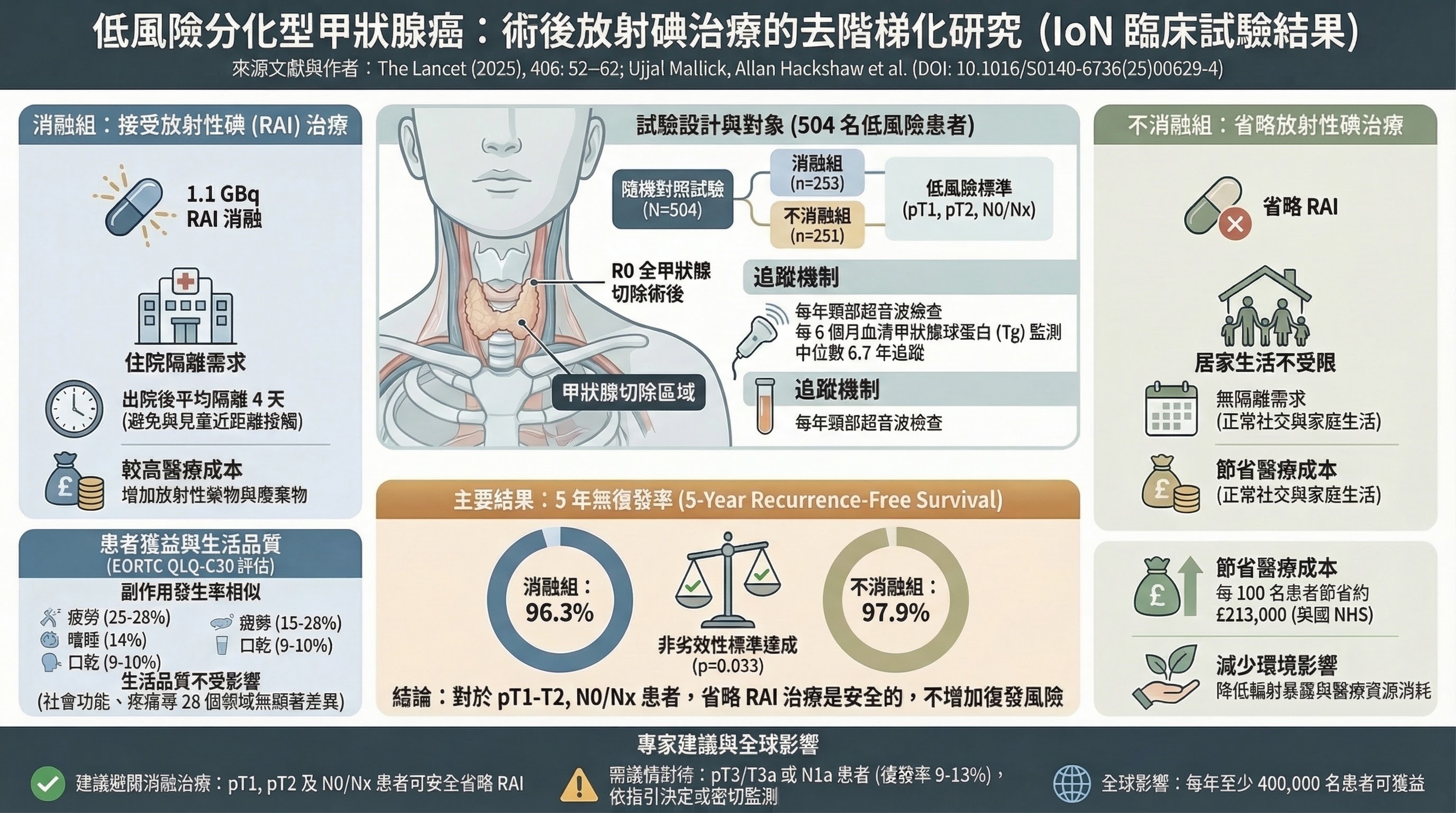
■ 關鍵文獻:IoN Trial(PMID: 40543520)
- Citation: Mallick U et al., Lancet, 2025; 406(10498):52–62
- 研究設計: National, multicentre, non-inferiority, open-label RCT,33 個英國癌症中心,N=504(251 no-ablation;253 ablation)
- PICO: P=完全切除(R0)DTC,pT1/pT2/pT3a,N0/Nx/N1a;I=術後無 ablation;C=1.1 GBq ablation(rhTSH 或 THW);O=5 年 recurrence-free survival
- 重要設計差異 vs ESTIMABL2: IoN 納入 pT2(2–4 cm)、部分 pT3a(microscopic ETE)及 N1a 患者;以臨床 RFS 為主要終點(非複合生物學終點)
- 主要發現:
- 5 年 RFS(ITT):No ablation 97.9%(95% CI 96.1–99.7)vs Ablation 96.3%(95% CI 93.9–98.7),差異 0.5%(95% CI -2.2 to 3.2),p_non-inferiority=0.033(ITT 達標)
- 5 年 RFS(per-protocol):No ablation 97.9% vs Ablation 96.9%,p_non-inferiority=0.093(未達標)
- 17 例復發:No ablation 8 例,Ablation 9 例
- ⚠️ 重要方法論說明: 試驗設計以 ITT 為主要分析(p=0.033 達標),per-protocol 未達標(p=0.093)是重要的方法論限制,應在引用時明確說明
- 為什麼支持此 recommendation 變更: ESTIMABL2 之外的獨立確認,且在更廣泛的患者(含 pT2 和 N1a)中同樣顯示非劣效性;兩項試驗合計強化跨國、跨患者特徵的適用性
- 主要限制: Open-label;pT3/N1a 亞組樣本數過小(每組 <25);中位追蹤約 6.8 年仍非終身
影響族群
所有 total thyroidectomy 後的 low-risk DTC 患者。估計佔 total thyroidectomy DTC 患者的 40–50%。
臨床實務調整
- 核醫/內分泌科: 停止對 low-risk DTC 常規使用 RAI;此決定有兩個 Phase 3 RCT 作為依據
- RAI 準備方式: rhTSH preparation 現為 preferred(R34A,Strong/High certainty),取代 thyroid hormone withdrawal(此為 2025 guideline 另一項 Strong/High 升級)
- 保留 RAI 使用的情境(select cases): Extensive vascular invasion(FTC/OCA ≥4 foci)、大量 pN1a 或 pN1b、BRAF+TERT co-mutation、分子高風險特徵
- 接受缺乏 post-therapy WBS staging 資訊的取捨(放棄 RAI 也意味著放棄 post-therapy whole-body scan)
連結到具體 Recommendation 變更
- R32A(low-risk DTC 不使用 RAI:Weak/Low → Strong/High)← ESTIMABL2 + IoN 雙 RCT
- R32B(intermediate-risk DTC 的 RAI 決策) R32B 的推薦強度為 Conditional/Low certainty evidence(非 Moderate)。Low-intermediate 和 intermediate-high 兩個 sub-tier 共用同一個 Conditional/Low "may be considered" 推薦,並無獨立的 stronger directive。這反映了 intermediate-risk RAI 領域 RCT 證據的根本缺乏:ESTIMABL2 和 IoN 均排除了 N1b、pT3b、pT4a 等高風險特徵的患者——恰恰是構成 intermediate-high 分類的核心族群。因此,2025 guideline 雖然能對 low-risk 做出 Strong/High 的反向推薦,卻只能對 intermediate-risk 給出 Conditional/Low 的不確定性推薦,指出 RAI「may be considered」並需 SDM。
- R33(RAI therapy 的適應症更明確)← 風險效益重新校準
- R34A(rhTSH 從 "alternative" 升為 "preferred":Strong/High certainty)← 當需要 RAI 時,rhTSH 的等效性及 QoL 優勢已有 Level I 證據支持
- R41(RAI 二次惡性腫瘤風險的 counseling 要求加強)← Kim 2023 dose-response data
注記
- 與 lobectomy 擴展的複合效應: Lobectomy 患者不符合 RAI 資格;更多 lobectomy + low-risk 強力反對 RAI = RAI 總量可能減少 40–60%
3. 預防性 Central Neck Dissection:從「不做也可以」到「不應該做」
變更概述
2015 guideline 以雙重否定的措辭表達了對不做 pCND 的接受(R36C: "thyroidectomy without prophylactic central neck dissection is appropriate", Weak/Low)。2025 guideline 轉為明確的否定(R19A: "prophylactic CND should not be performed for most patients with T1-T2 cN0 PTC", Strong/Moderate)。
變更內容
| 2015 | 2025 | |
|---|---|---|
| R36C | 對 T1–T2 cN0 PTC 不做 pCND「is appropriate」(Weak/Low) | — |
| R19A | — | pCND「should NOT be performed」對多數 cT1–T2 cN0 PTC(Strong/Moderate certainty) |
| Change type | 從「可省略」升格為「強推薦不做」 | strengthened directive against |
變更原因
2025 guideline 引用 meta-analysis 量化的 harm-benefit tradeoff,明確顯示 morbidity 超過邊際 LRR 降低的代價。
關鍵文獻
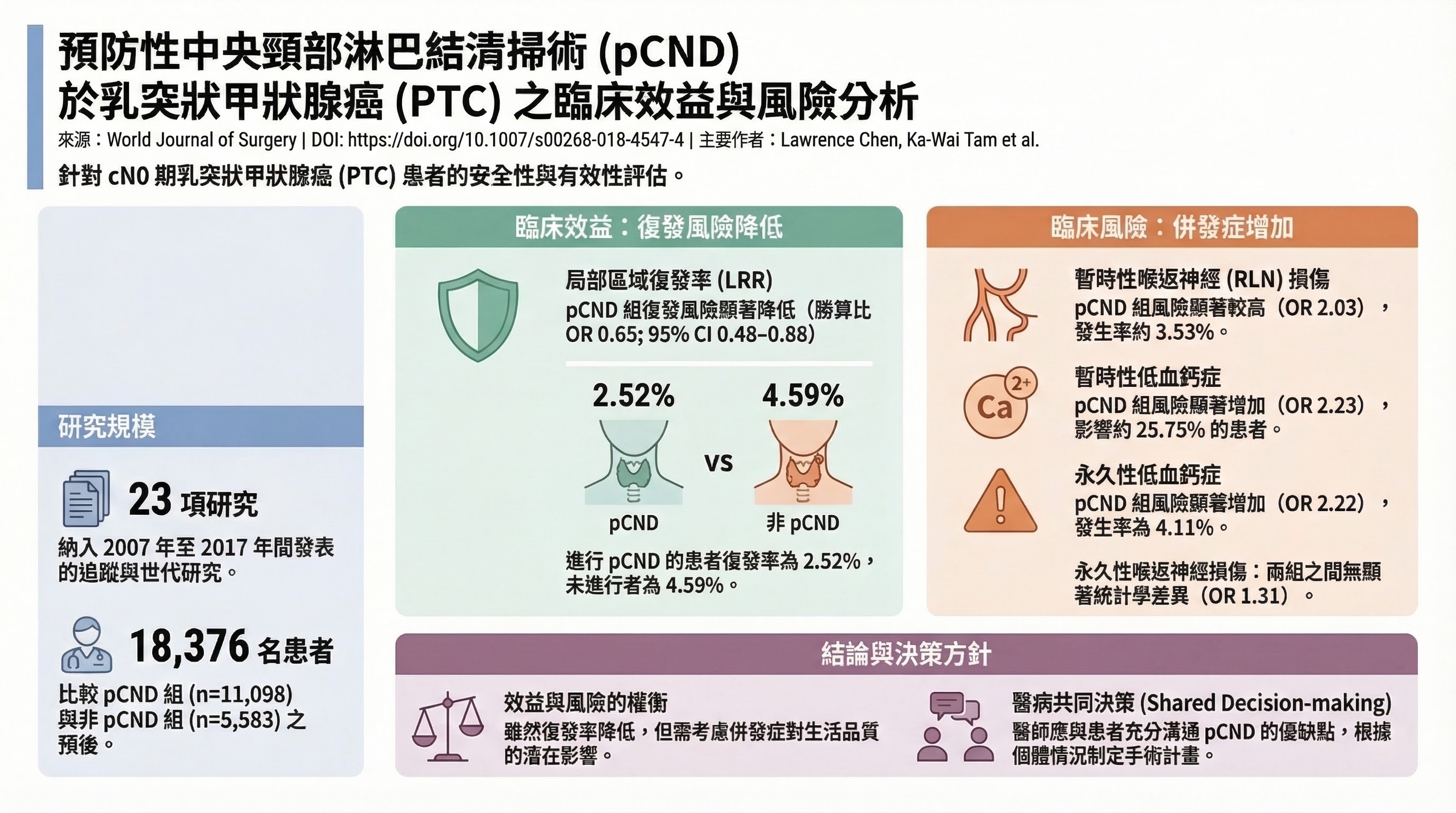
■ 關鍵文獻:Chen et al. 2018(PMID: 29488066)
- Citation: Chen L et al., World J Surg 2018;42(9):2846–2857
- 研究設計: Systematic review and meta-analysis,23 項研究(總 N=18,376),文獻截止 2017 年 9 月;PROSPERO 登記(CRD42017069976)
- PICO: P=cN0 PTC(接受 TT),I=TT+pCND,C=TT alone,O=LRR,transient/permanent RLN injury,transient/permanent hypocalcemia
- 主要發現:
- LRR(20 項研究):pCND 組 2.52% vs 無 pCND 組 4.59%;OR=0.65(95% CI 0.48–0.88)— 統計顯著
- Transient hypocalcemia:OR=2.23(CI 1.84–2.70)— 顯著增加
- Permanent hypocalcemia:OR=2.22(CI 1.58–3.13)— 顯著增加
- Transient RLN injury:OR=2.03(CI 1.32–3.13)— 顯著增加
- Permanent RLN injury:OR=1.31(CI 0.75–2.27)— 無顯著差異
- 效益解讀: LRR 絕對差異約 2%(4.59% → 2.52%),NNT ≈ 31–50 才能預防 1 次復發;然而 pCND 組接受更高劑量 RAI(74.6% vs 59.9%),意味著 LRR 降低可能部分由 RAI 差異所致,而非 pCND 本身
- 為什麼支持此 recommendation 變更: 最大規模的 pCND meta-analysis,確認了 harm-benefit tradeoff:LRR 降低的絕對效益(約 2%)遠小於 permanent hypocalcemia 風險加倍(OR 2.22)的代價
- 主要限制: 全部為觀察性研究;selection bias;LRR 定義不一致;多數患者均接受 RAI,混淆 pCND 純粹效益
其他支持文獻:
- Wang TS 2013 meta-analysis:pCND 復發 RR 0.59(95% CI 0.33–1.07,跨越 1.0,未達統計顯著),NNT=31
- Wang Y 2023 meta-analysis:permanent hypocalcemia OR=4.24(95% CI 1.05–17.22,P=0.043,CI 極寬,邊際顯著性,需謹慎解讀)
- Hughes et al.(14 項研究):「observation of the central neck is safe」
Guideline 委員會的判斷: 2025 guideline 原文承認「All these studies suggest equipoise when considering a pCLND, especially with T3 and T4 tumors」,但委員會基於 harm-benefit 分析判斷給予 Strong recommendation against——比引用文獻本身更為強硬的立場。
影響族群
約 60–70% PTC 患者(cT1–T2 cN0)。Strong recommendation 為外科醫師提供了更有力的依據,也影響相關醫療法律定位。
連結到具體 Recommendation 變更
- R19A(T1-T2 cN0 不做 pCND:Weak/Low → Strong/Moderate)← meta-analyses 量化 risk-benefit
- R28(4-tier risk system:microscopic N1a 降至 low-intermediate)← 減少 pCND-driven upstaging 的影響
臨床實務調整
- 外科醫師: 停止對 T1–T2 cN0 PTC 常規行 pCND(Strong recommendation 提供強力依據)
- 對 T3–T4 cN0 患者(R19B): pCND「may be considered」(Conditional/Low);應依個別風險因子決定,並明確說明適應症
- 病理科: 執行 CND 時,synoptic report 應包含 examined lymph node 數量(≥5 顆 central;≥20 顆 lateral)、LNR、extranodal extension
- Tumor board: 不要以 pCND 偶然發現的 microscopic pN1a disease 作為啟動 RAI 的唯一理由
4. 術後風險分層:3 級 → 4 級系統(RAI 和 TSH 決策精細化)
變更概述
2015 guideline 使用三層 ATA risk system(Low / Intermediate / High)。2025 guideline 將 Intermediate 分拆為 Low-Intermediate 和 Intermediate-High,建立四層系統。
變更內容
| 2015 | 2025 | |
|---|---|---|
| Risk tiers | 3 級:low / intermediate / high | 4 級:low / low-intermediate / intermediate-high / high |
| Intermediate 類別 | 單一層級(復發風險 5–20%,異質性高) | 拆分:low-intermediate(5–10%)vs intermediate-high(10–25%) |
| OTC | 視為 FTC 變體 | 獨立 DTC 實體,有自己的 risk stratification |
變更原因
2015 intermediate 類別涵蓋風險差異極大的患者群:microscopic N1a 復發率 4–8%,macroscopic disease >20%。AJCC 8th 版移除 microscopic ETE 的 T3 效應(30–40% PTC 降期)。Ghossein 2006、Leong 2022、Ito 2022 確認 vascular invasion foci 數量(<4 vs ≥4)的預後意義,支持 FTC/OCA 更精細分層。
關鍵文獻
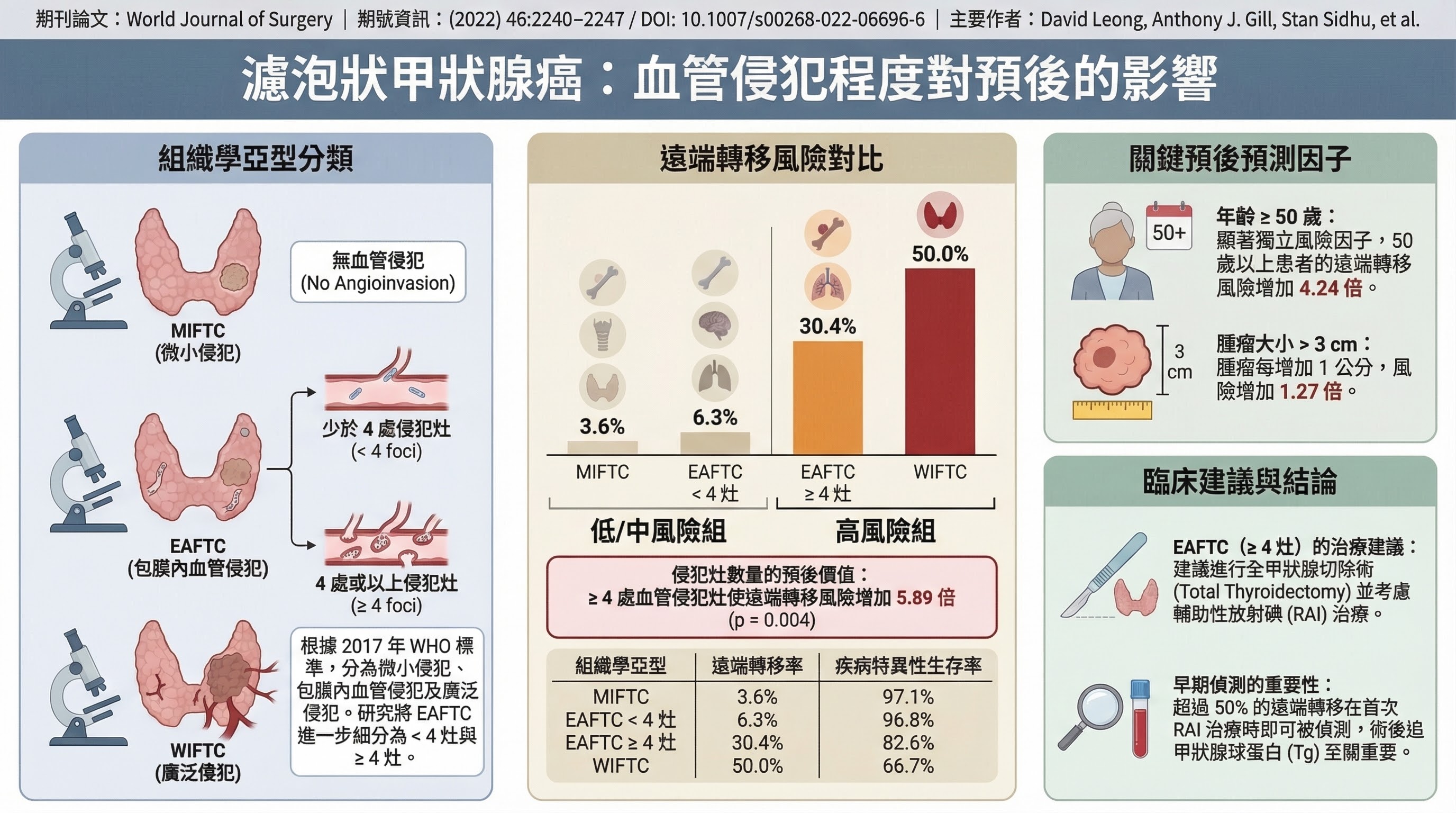
■ 關鍵文獻:Leong 2022(PMID: 36031639)
- Citation: Leong A et al., Thyroid 2022;32(12):1564–1571
- 研究設計: 回溯性多中心研究,N=292 FTC
- 主要發現: ≥4 foci vascular invasion:遠端轉移 HR 5.89(P=0.004),DSS 82.6% vs 96.8%;<4 foci:遠端轉移風險 6.3%
- 為什麼支持此 recommendation 變更: 確立 ≥4 foci 的 cut-off 作為 extensive angioinvasion 的定義,直接支持 2025 年 intermediate-high risk 的界定
影響族群
所有先前歸類為「intermediate risk」的患者——人數最多且臨床異質性最大的群體。RAI、TSH suppression 和 surveillance 決策均源自風險分層。
重要限制(Figure 2 腳註): 2025 guideline 本身承認「No clear cutoffs for LNs between low-intermediate and high-intermediate risk groups」——4 級系統的邊界在 lymph node 數量方面仍存在任意性。
連結到具體 Recommendation 變更
- R28(4-tier risk stratification)← Intermediate heterogeneity + AJCC 8th + WHO 2022
- R32-33(RAI 決策精準化)← 依四層分類而非三層
- R45-46(TSH suppression 個體化)← 依四層分類決定 TSH target
臨床實務調整
- 病理報告: 確保 synoptic reports 包含 lymph node 數量、LNR、extranodal extension、vascular invasion foci 計數、OTC 狀態
- EMR 模板: 從 3 級更新為 4 級 risk stratification
- 術語更新: OTC 取代 Hurthle cell carcinoma(WHO 5th edition)
- Tumor board: 明確將原「intermediate」患者分入 low-intermediate 或 intermediate-high,此分類驅動 RAI 和 TSH 決策
5. TSH 抑制動態化:靜態 Initial Risk → Dynamic Response-to-Therapy
變更概述
2015 guideline 對 high-risk 患者推薦 TSH <0.1 mU/L(Strong),低風險 excellent response 患者推薦 TSH 0.5-2 mU/L。2025 guideline 弱化了 suppression 的推薦(R45, Conditional/Low),並明確建議低和中風險無復發患者不進行長期 TSH suppression(R46A)。
變更內容
| 2015 | 2025 | |
|---|---|---|
| 決策依據 | 依初始 ATA 風險設定靜態 TSH 目標(3 個分離 recommendations) | 依動態治療後反應(DRS)設定 TSH 目標(R45/R46) |
| Excellent response | Low risk:0.5–2 mU/L;High risk:<0.1 mU/L | Excellent response → 0.5–2 mU/L(無論初始風險) |
| Long-term suppression(low/intermediate risk,無復發) | 靜態(依風險層) | R46A:不建議(Conditional/Low) |
關鍵文獻
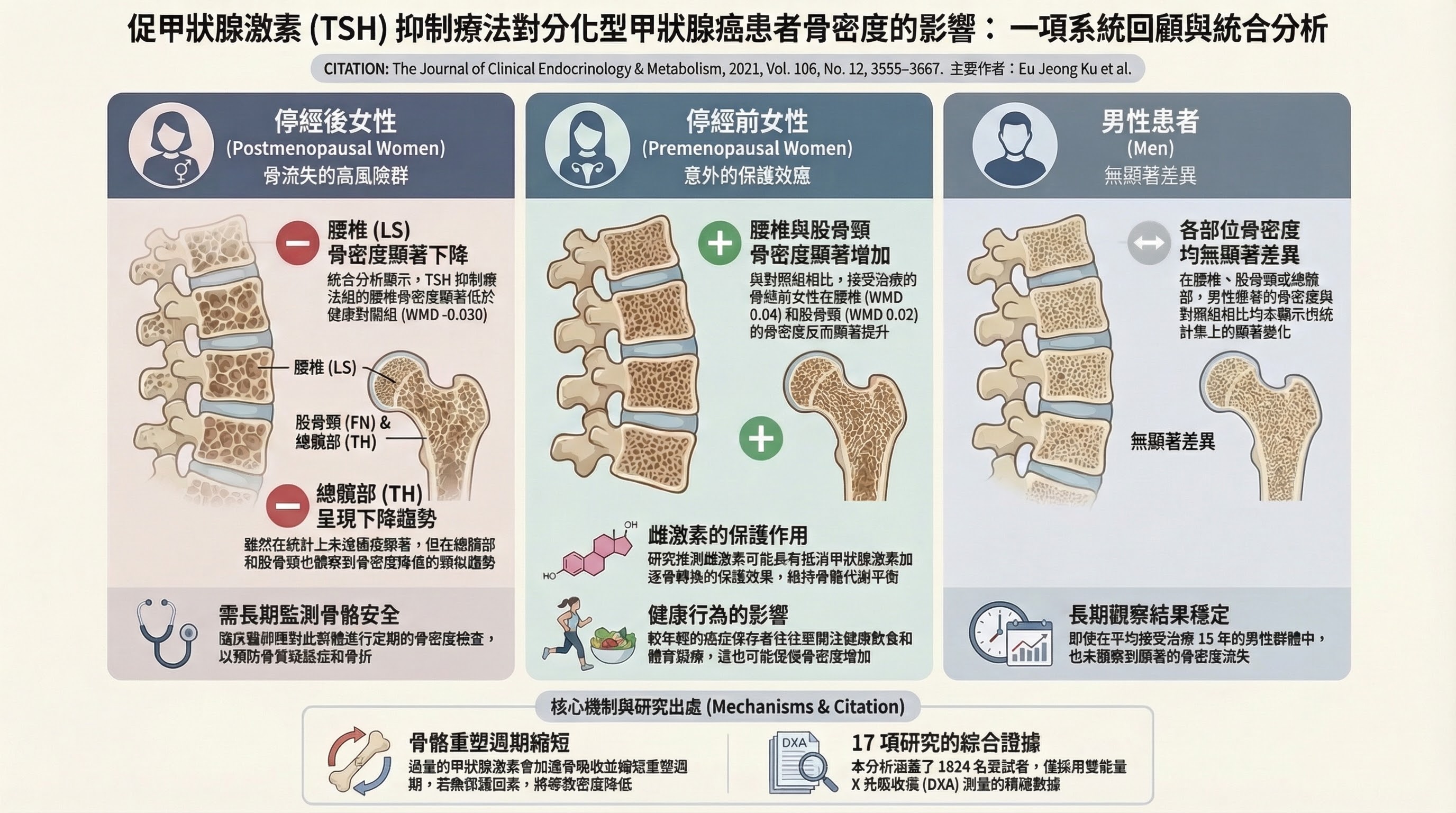
■ 關鍵文獻:Ku et al. 2021(PMID: 34302730)
- Citation: Ku EJ et al., J Clin Endocrinol Metab 2021;106(12):3655–3667
- 研究設計: Systematic review and meta-analysis,20 項研究(17 進入定量分析),N=739 患者 + 1,085 對照
- 主要發現: 停經後女性 lumbar spine BMD:WMD -0.030 g/cm²(95% CI -0.050 to -0.020,P<0.001)——顯著下降;停經前女性 lumbar spine BMD:WMD +0.040(P<0.001)——顯著上升;男性:無顯著差異
- Subgroup by duration: <5 年和 >5 年 TSH 抑制的亞組分析無明顯差異,提示骨質流失較早發生
- 為什麼支持此 recommendation 變更: 量化了 TSH 抑制對停經後女性骨質的確定性傷害,支持對 excellent response 患者放鬆 TSH 目標
- 主要限制: 全部為觀察性研究;I²=73% 代表高度異質性;無骨折事件資料(僅 BMD 替代指標)
■ 關鍵文獻:Seejore et al. 2021(PMID: 34185343)
- Citation: Seejore K et al., Clin Endocrinol 2021;96(3):395–401
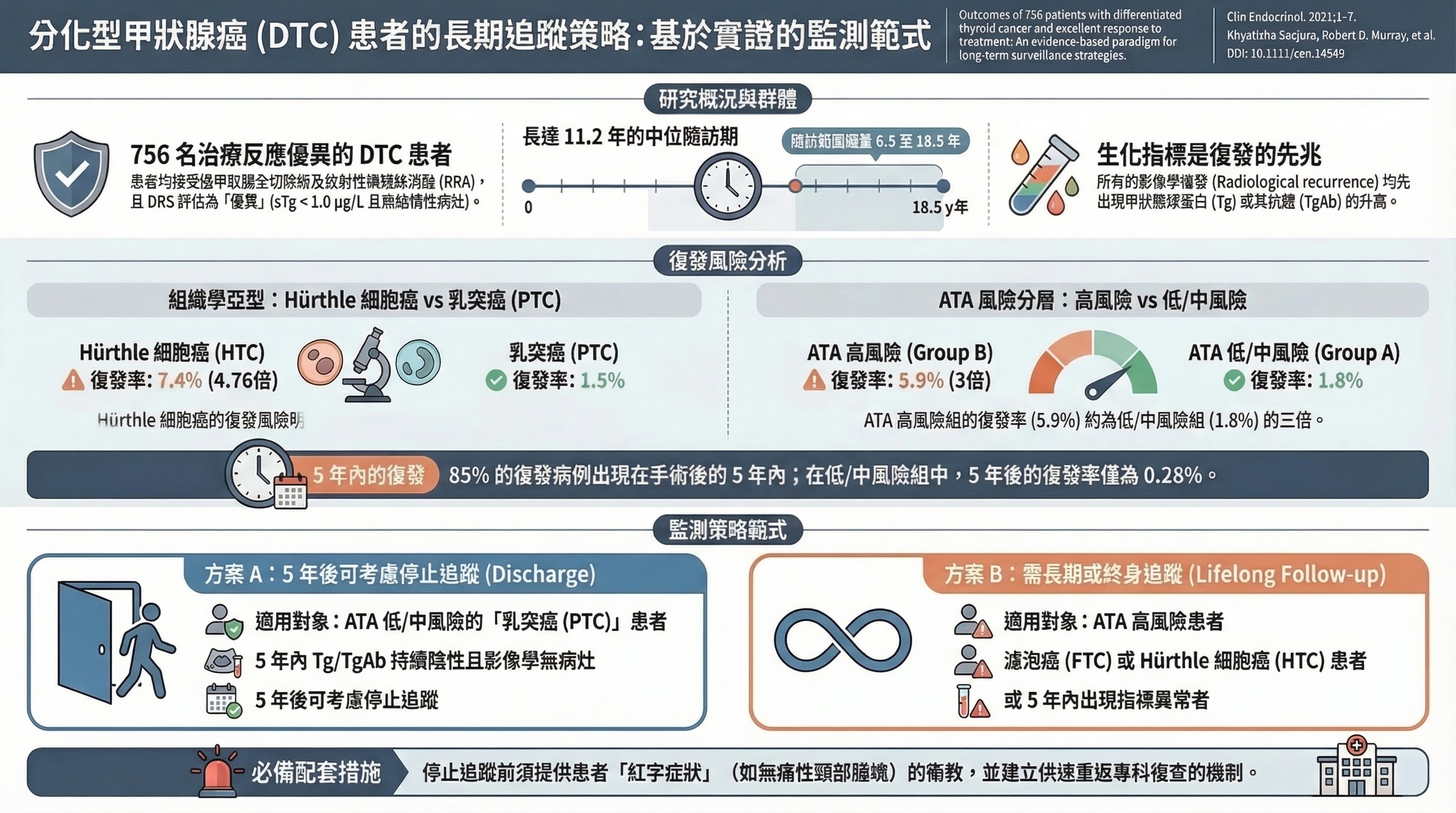
- 研究設計: 單中心回溯性 cohort,Leeds Cancer Centre,N=756(TT + RRA,DRS excellent response);中位追蹤 11.2 年
- 主要發現: 15/756(2.0%)發生放射學復發;ATA 低/中風險組 5 年後新增復發率僅 0.28%(2/722);所有復發均由 Tg/TgAb 先行識別(平均提前 7 個月)
- HTC(OTC)的特殊情況: OTC 復發率 5/68(7.4%)vs PTC 9/582(1.5%);RR 4.76(95% CI 1.64–13.8)——說明 OTC 患者即使達 excellent response 也不應適用停止監測標準
- 為什麼支持此 recommendation 變更: 在 excellent response 患者中,5 年後復發極少且均先有生化預警,支持放鬆 TSH 抑制目標並降低監測強度
- 主要限制: 單中心(英國);全部接受 TT + RAI(不適用於 lobectomy 患者);使用 BTA 而非 ATA 標準
連結到具體 Recommendation 變更
- R45(TSH suppression 個體化:Strong → Conditional)← NTCTCSG + 心血管/骨骼 harm data
- R46A(低/中風險無復發者不建議長期 TSH suppression)← 同上
- 此變更與 lobectomy 擴大密切相關:lobectomy 後約 70-80% 患者可維持正常甲狀腺功能而無需外源性甲狀腺激素
影響族群
數十萬名 DTC 存活者(TSH 動態化),以及所有已達 excellent response 的長期追蹤患者(surveillance 終點)。
臨床實務調整
- 確認 excellent response 後: 將 TSH 目標調整至正常範圍(0.5–2 mU/L);不需終身 TSH 抑制
- Post-lobectomy: 術後 6–8 週檢測 TSH;若正常,不開始 L-T4;70–80% 的 lobectomy 患者可完全保留功能
- 年長者、停經後婦女: Ku 2021 確認 TSH 抑制對骨質的確定性傷害,應積極評估放鬆 TSH 目標
- OTC 患者: 即使達 excellent response,監測降階需謹慎(RR 4.76 vs PTC)
6. 監測終點定義:5–8 年 US,10–15 年「Complete Remission」
變更概述
2015 guideline 未定義 follow-up 的終點——surveillance 本質上是終身的。2025 guideline 首次引入了「complete remission」概念(R48),定義了 US 監測可於 5-8 年後停止、生化監測可於 10-15 年後停止的 stopping rules。
變更內容
| 2015 | 2025 | |
|---|---|---|
| US 終點 | 未定義;「periodically」 | 持續 excellent response 5–8 年後可停止(R48.1, Conditional/Low) |
| Tg 終點 | 未定義;持續 q6–12 個月 | 10–15 年後可達「complete remission」(R48.2, GPS) |
| Lobectomy 後 Tg | 定期常規(R64, Strong/Low) | 不建議常規(R47D, Conditional/Very low) |
| Lobectomy 後路徑 | 未區分 | US q1–3 年持續 5–8 年;不進入 complete remission 路徑(GPS) |
⚠️ 註記: Complete remission(10–15 年停止 Tg 監測)路徑僅適用於 total thyroidectomy 患者(with or without RAI)。Lobectomy 患者進入不同路徑(R48.5/R48.6,GPS level),不定義 complete remission 終點。
變更原因
Seejore 2021(N=756,中位追蹤 11.2 年):excellent response 後 5 年新增復發率 0.28%,且所有復發均由 Tg/TgAb 先行識別;持續密集監測缺乏改善結果的證據,消耗資源並增加焦慮。Lobectomy 後 Tg 不可靠(完整對側甲狀腺葉存在時,無法作為腫瘤標記)。
影響族群
目前處於無限期監測中的數十萬 DTC 存活者。這是 guideline 中所有 recommendation 變更影響族群最大的項目之一。
臨床實務調整
- Total thyroidectomy 後 excellent response 5–8 年: 討論停止常規 US(Conditional/Low)
- Total thyroidectomy 後 excellent response 10–15 年: 引入「complete remission」概念並討論停止 biochemical monitoring
- Lobectomy 後: 術後約 12 週取得單次 Tg;若不顯著升高,不計畫常規 serial Tg;以 US q1–3 年追蹤 5–8 年為主要監測工具
- 停止監測的條件: 僅適用於 TT(±RAI)後達 sustained excellent response;Indeterminate、incomplete response 或 OTC 患者請勿停止
7. Active Surveillance 正式獲得背書(從 2015 R12 提升)
變更概述
2015 guideline 在結節章節(R12)提及 active surveillance(AS)的可能性,但在 DTC 章節中無獨立 recommendation。2025 guideline 正式將 AS 確立為 cT1aN0M0 PTC 的管理選項(R11, Conditional/Low),並新增了 percutaneous ablation 作為替代選項(R11B),同時標準化了 AS 監測方案(R12-14)。
變更內容
| 2015 | 2025 | |
|---|---|---|
| 位置 | R12(nodule section):AS「can be considered」,主要針對高手術風險患者(Weak/Low) | R11A(DTC section):AS「may be offered」for cT1aN0M0 PTCs(Conditional/Low) |
| 適用範圍 | 主要為手術高風險、有限壽命、合併症 | 擴大:透過 shared decision-making 向一般低風險 microcarcinoma 患者開放 |
| R11 formal scope | — | cT1aN0M0(≤1 cm);1–2 cm 的建議存在於討論段落,非 recommendation 原文 |
深層理據
(一)30 年追蹤的長期安全性數據。 AS 的證據基礎主要來自日本兩大中心(Kuma Hospital 和 Cancer Institute Hospital)的前瞻性觀察研究,以及近年來韓國和西方國家的驗證性研究。
■ 關鍵文獻:Miyauchi & Ito 2023 Kuma Hospital 30-Year Data
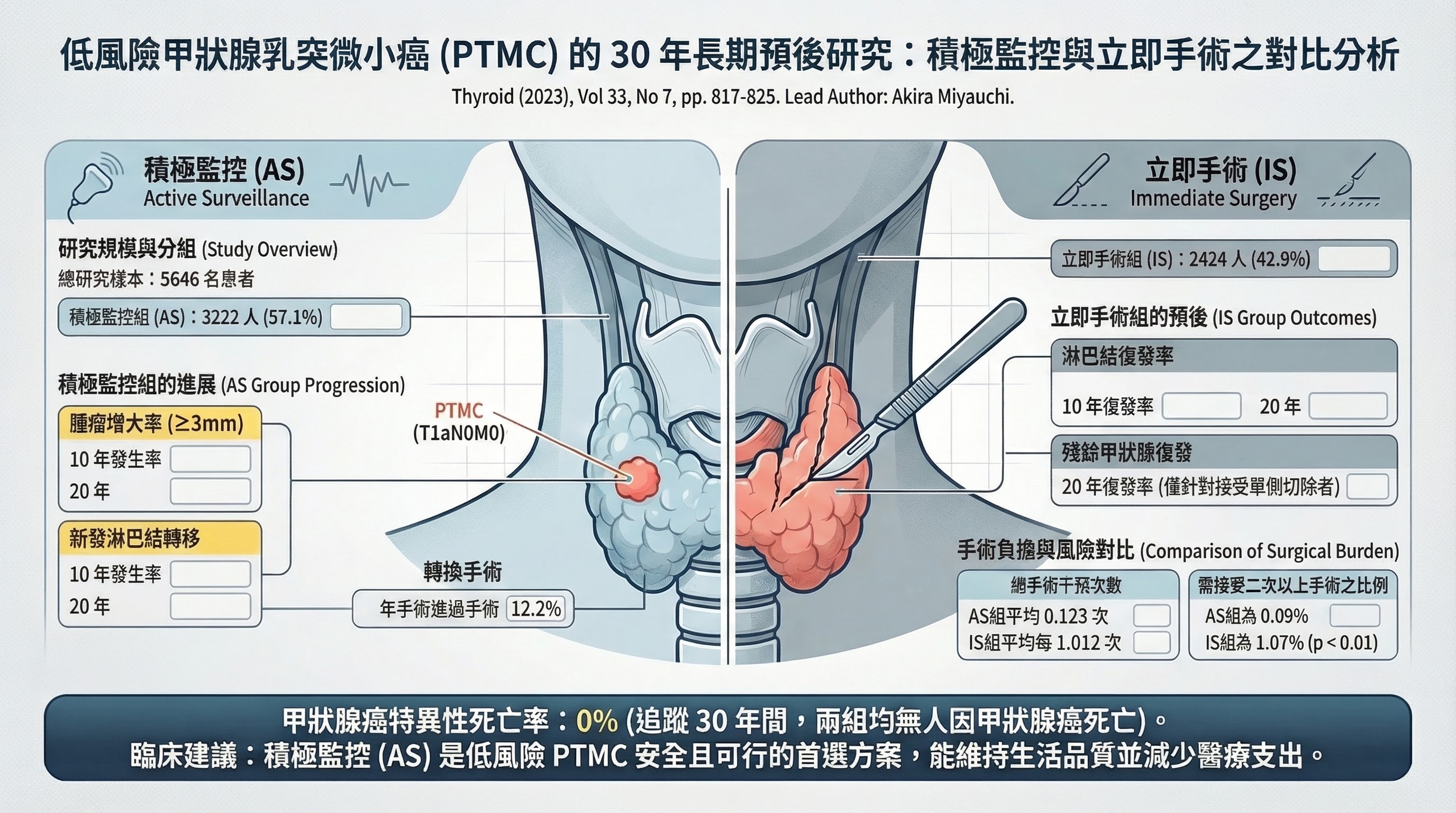
- Citation: Miyauchi A, Ito Y, Fujishima M, et al. Thyroid, 2023; 33(7):817-825 (PMID: 37166389)
- 研究設計: Retrospective cohort, N=5,646 (3,222 AS, 2,424 immediate surgery), follow-up up to 30 years
- PICO: P=papillary thyroid microcarcinoma (<=1 cm); I=active surveillance; C=immediate surgery; O=tumor progression, LN metastasis, disease-specific mortality
- 主要發現: 10 年腫瘤增大率僅 4.7%,20 年增大率 6.6%。10 年淋巴結轉移率 1.0%,20 年 1.6%。30 年追蹤期間無一人死於甲狀腺癌。由 AS 轉為手術者的預後與立即手術者完全相同。
- 為什麼推動了 guideline 的方向性轉變: 這是全球最大且追蹤最長的 AS 世代研究。「30 年零疾病特異性死亡」的數據為 AS 的安全性提供了近乎終極的證據。此研究亦證明延遲手術不影響預後——這是患者選擇 AS 時最關切的問題。Ito 和 Miyauchi 自 2003 年發表首份 AS 報告(PMID: 12804106)以來,持續追蹤並擴大樣本,經過 20 年建構了一個無法被否認的 evidence base。
(二)跨文化外部效度的建立。 日本數據的一個合理質疑是:日本人群的甲狀腺癌生物學行為和醫療環境是否可推廣至其他人群?KoMPASS 研究和 Tuttle 領導的西方 AS 實踐部分回答了此問題。
■ 關鍵文獻:Lee et al. 2022 KoMPASS
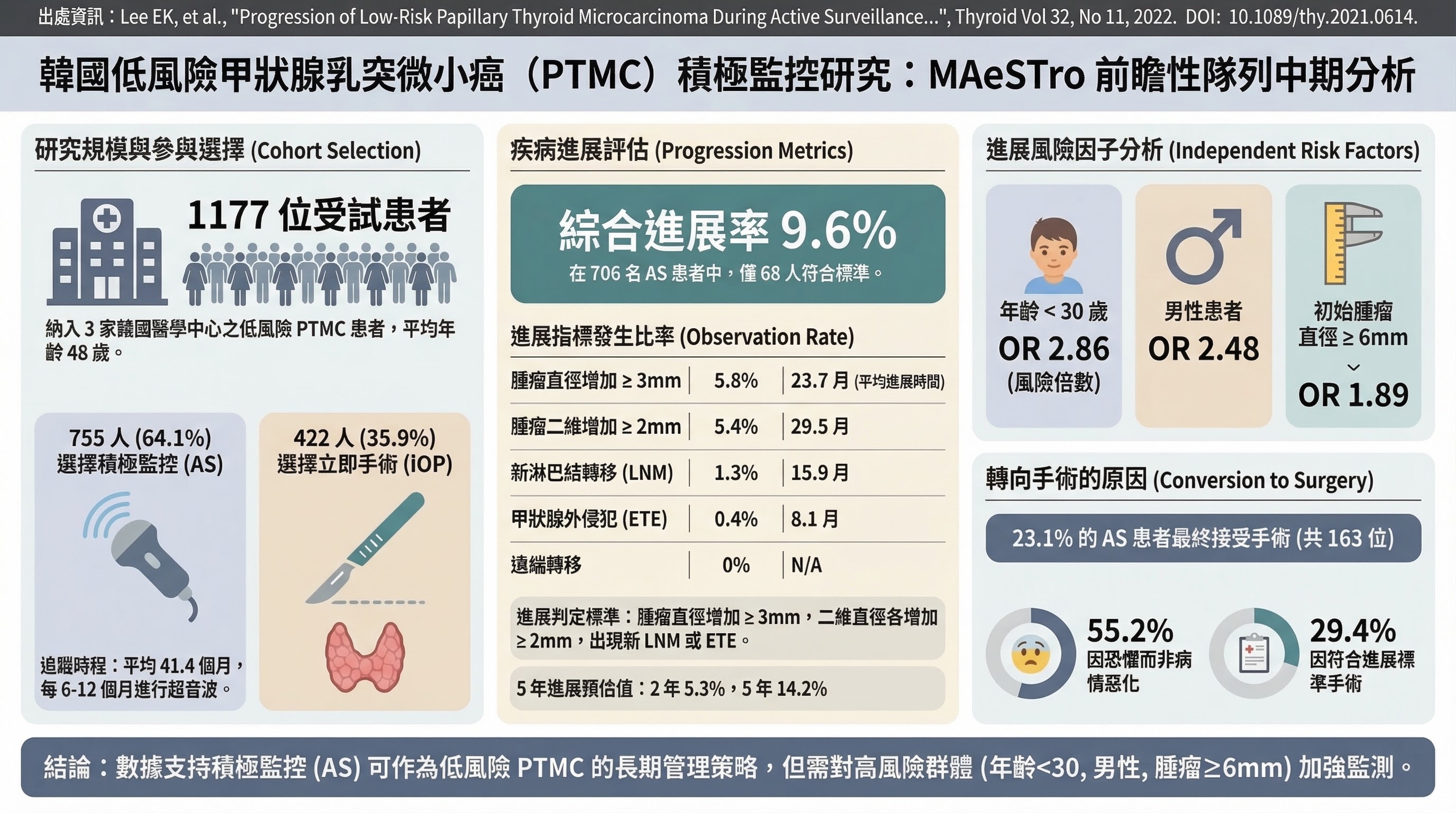
- Citation: Lee EK et al., Thyroid, 2022; 32(11):1328-1336 (PMID: 36205563)
- 研究設計: Multicenter prospective cohort, N=755 (AS) vs 422 (surgery), Korea
- 主要發現: 5 年進展率 14.2%(略高於日本數據)。進展風險因子:age <30(OR 2.86)、male sex(OR 2.48)、tumor >=6mm(OR 1.89)。ZERO distant metastasis during AS。
- 為什麼推動了 guideline 的方向性轉變: 首個大規模非日本前瞻性 AS 數據。雖然進展率高於日本(14.2% vs ~5%),但零遠處轉移的結果仍確認了 AS 的安全性。人群差異(如年齡、性別等風險因子的辨識)有助於 guideline 制定者理解 AS 的適用範圍與限制。
(三)Overdiagnosis 概念在 PTMC 中的具體化。 AS 的興起與 overdiagnosis 敘事高度同構:如果大部分被偵測到的 PTMC 本來就不會造成傷害,那麼對它們進行手術便是 overtreatment。AS 是 overdiagnosis 問題在臨床層面的解決方案——你不能「un-diagnose」一個已被告知的癌症,但你可以選擇不立即治療它。2025 guideline 藉由正式納入 AS,從制度層面承認了 overtreatment 的存在。
剩餘不確定性
AS 尚有數個未解問題:(1) 最佳 conversion-to-surgery criteria 尚未標準化(腫瘤增大多少才需手術?3 mm 增長的定義可靠嗎?);(2) 患者心理層面的影響——AS 雖然避免了手術併發症,但「與癌共存」的焦慮可能同樣影響 QoL(Sawka et al. 2024, PMID: 38481111 顯示 AS 與手術在焦慮和憂鬱程度上無顯著差異,但需更多長期數據);(3) 在尚未建立成熟 AS program 的醫療機構中推行 AS 的可行性和安全性。
連結到具體 Recommendation 變更
- R11A(AS 正式成為 cT1aN0M0 PTC 的管理選項)← Kuma 30 年數據 + KoMPASS + 西方驗證
- R11B(percutaneous ablation 作為替代)← AS 概念的延伸 + 新技術
- R12-14(AS 監測方案標準化)← 實施層面的需求
影響族群
Papillary thyroid microcarcinoma(cT1aN0M0)患者,尤其年長(>60 歲)患者。
臨床實務調整
- 建立院內 AS protocols: US q6 個月 x 1–2 年,之後每年;定義手術觸發條件(growth ≥3 mm、new LN mets、ETE、patient anxiety)
- 擴大候選範圍: 透過適當 SDM,不限於手術禁忌症患者
- 記錄排除標準: aggressive histology、ETE/invasion、lateral neck nodules、posteriorly located tumors abutting trachea
- 接受患者焦慮退出(10–30% 患者因焦慮選擇手術)
8. cT2(2–4 cm)的 Lobectomy:Conditional Preference(確定性較低)
變更內容
| 2015 | 2025 | |
|---|---|---|
| Recommendation | R35B: 「can be either a bilateral procedure... or a unilateral procedure」(Strong/Moderate) | R15B: Lobectomy「may be the preferred initial surgical treatment」(Conditional/Low-moderate) |
| Change type | 從真正的 clinical equipoise | 方向性偏好 lobectomy,但確定性降低 |
此項刻意排在第 8 位,因為確認顯著的不確定性。 約半數 meta-analyses 顯示 cT2 腫瘤 total thyroidectomy 有較低復發率(特別是 classical PTC)。Recommendation strength 從 Strong/Moderate 降為 Conditional/Low-moderate,反映真實的數據矛盾。
變更原因
Rajjoub 2018 對 conventional PTC 2.0–3.9 cm 發現 TT 有邊際存活優勢(HR 1.53, P=0.022),但 Song 2019 的 propensity-matched 研究顯示 HR 0.93(P=0.902)——數據衝突,合理的結論為 SDM,而非強制性建議。FVPTC 在兩項研究中均無差異。
臨床實務調整
- 記錄 SDM 討論: 需討論腫瘤大小、組織亞型(classical PTC vs FVPTC)、患者對 L-T4 的態度、是否預期需要 RAI、若術後發現 high-risk features 時 completion 的可能性
- Histotype 有影響: Lobectomy 偏好最確定地適用於 FVPTC;對 classical PTC cT2 最不確定
- Total thyroidectomy 仍為合理選擇(特別是患者偏好 RAI-based follow-up 時)
9. RAI-Refractory DTC 的 Precision Oncology(突變特異性靶向治療)
變更概述
2025 guideline 整合了 WHO 2022 classification(5th edition)、AJCC 8th edition staging、BRAF-like vs RAS-like 分子亞型概念,以及 RAIR DTC 的 mutation-specific targeted therapy(R61-72)。
變更內容
| 2015 | 2025 | |
|---|---|---|
| Framework | 1 項通用建議(sorafenib 或 lenvatinib) | 14 項 mutation-specific recommendations(R61–R74) |
| 藥物 | Sorafenib、Lenvatinib | + Larotrectinib(NTRK)、Selpercatinib(RET)、Dabrafenib+Trametinib(BRAF V600E)、ALK inhibitors |
| 決策邏輯 | 經驗性 MKI | Molecular testing 必要;gene-specific TKI 優先於廣譜 MKI |
關鍵文獻
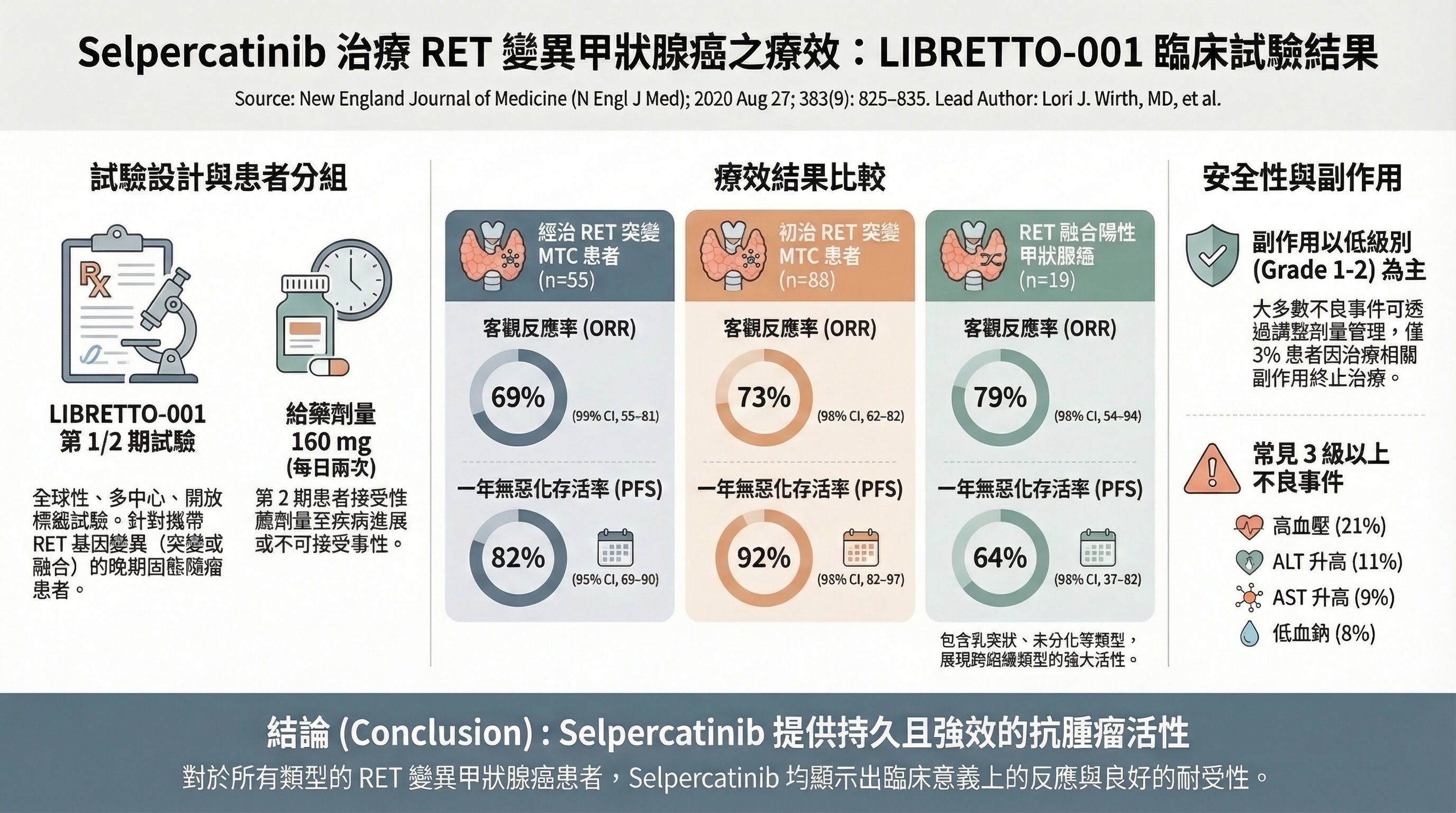
■ 關鍵文獻:LIBRETTO-001(PMID: 32846061)
- Citation: Wirth LJ et al., N Engl J Med 2020;383:825–835
- 研究設計: Phase 1/2 basket trial(selpercatinib for RET fusion-positive tumors)
- 主要發現: RET fusion-positive DTC ORR 79%(95% CI 54–94);1 年 PFS 82%;FDA 核准 selpercatinib 2020
- 為什麼支持此 recommendation 變更: RET fusion DTC 首次有 FDA 核准的精準靶向治療;ORR 79% 遠超廣譜 MKI
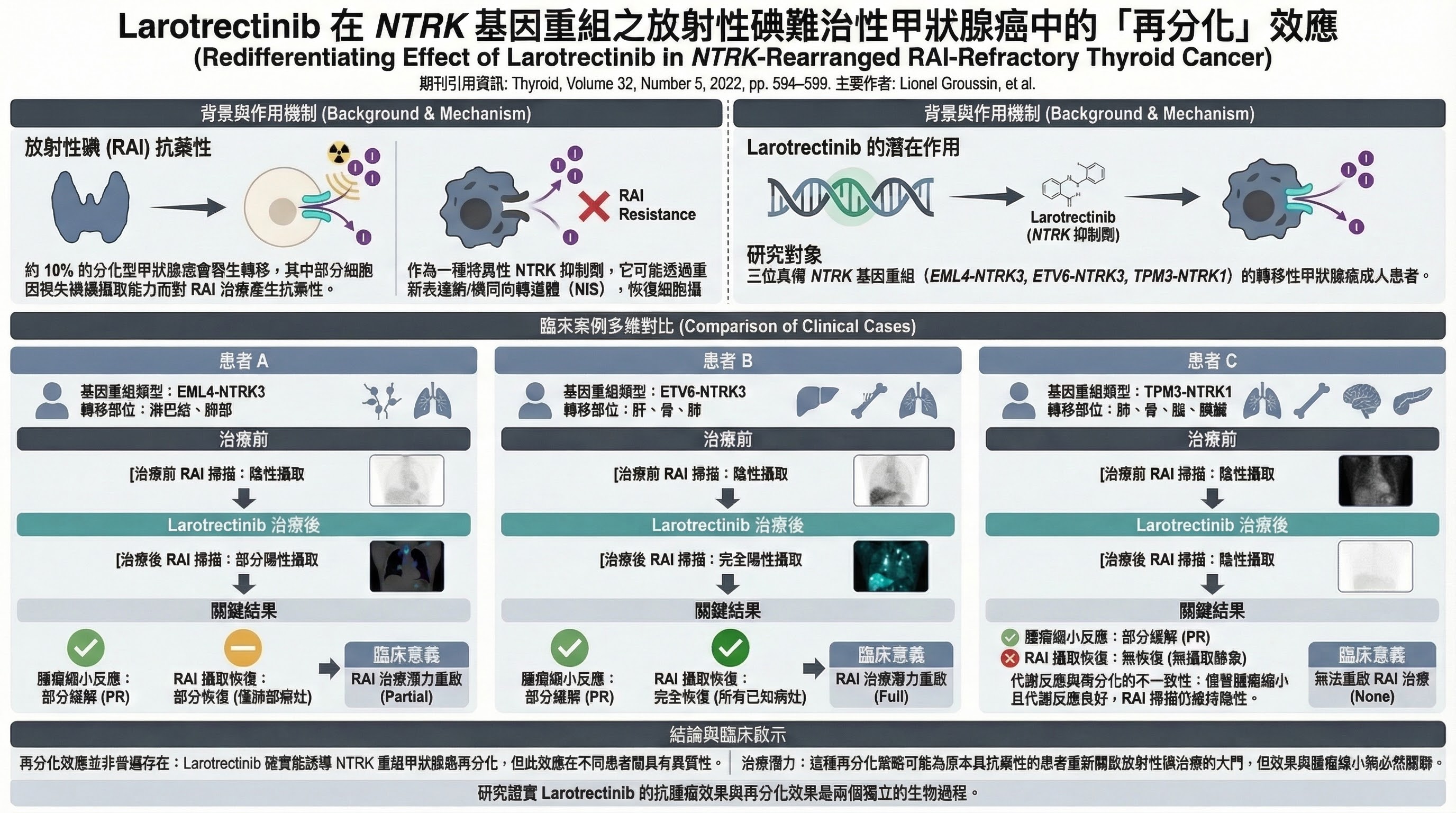
■ 關鍵文獻:Groussin et al. 2022(PMID: 35171708)
- Citation: Groussin L et al., N Engl J Med 2022
- 主要發現: Larotrectinib 在 NTRK fusion RAIR DTC 中誘導 redifferentiation(2/3 病例重新獲得 RAI avidity)
- 為什麼支持此 recommendation 變更: 建立了 redifferentiation 的概念——靶向治療不僅可縮小腫瘤,還可能恢復 RAI 敏感性
影響族群
Progressive RAI-refractory DTC 患者——雖絕對人數較少,但此亞群受益巨大。Molecular testing 成為開始全身性治療前的必要步驟。
臨床實務調整
- Molecular testing 現在對所有 RAIR DTC 患者在全身性治療前是必要的(NTRK、RET、BRAF V600E、ALK fusions)
- 發現 actionable mutation 時使用 gene-specific targeted therapy(優先於廣譜 MKI)
- 考慮 redifferentiation 策略: BRAF-mutated RAIR DTC 可嘗試 dabrafenib+trametinib 誘導 RAI 重新攝取
10. Completion Thyroidectomy 降級(Conditional 取代 Strong)
變更內容
| 2015 | 2025 | |
|---|---|---|
| Recommendation | R38A: 「Should be offered」若原本建議 TT(Strong/Moderate) | R16A: 「May be considered」依術後風險、RLN 狀態、患者偏好(Conditional/Low-moderate) |
| 決策框架 | 假設性:「如果事先知道,會不會做 TT?」 | 風險導向:「此患者的風險特徵是否從 completion 獲益?」 |
影響族群
因 indeterminate cytology 行 lobectomy 後被診斷為 DTC 的患者(常見臨床情境)。低風險患者多數可觀察,不再需要 completion thyroidectomy。
臨床實務調整
- 使用 2025 年 4-tier risk stratification 評估: Low risk(≤2 cm,無 aggressive features,無 ETE,低體積 LN)→ 衛教 lobectomy 可能已足夠
- 明確的 completion 觸發條件: pN1b、多發 pN1a(>5 nodes 或 extranodal extension)、extensive vascular invasion(FTC/OCA ≥4 foci)、BRAF+TERT co-mutation、gross ETE、患者偏好 RAI-based follow-up
- 記錄: LNR、VI foci 計數、RLN 功能狀態、患者偏好
11. Shared Decision-Making (SDM) 形式化
The Change
2015 年 SDM 在 Aim section 被提及但未嵌入個別 recommendations。2025 年 SDM 語言明確整合於 R11(AS)、R15B(lobectomy vs TT for T2)、R16(completion thyroidectomy)、R45(TSH suppression)等多項 recommendations 中,並在 initial management overview(p.855)中以結構化方式呈現。
What the Guideline Says About Why
2025 guideline(p.855):
"Shared decision-making between patients and their treating clinicians is paramount in determining the goals of initial therapy for patients with DTC."
Guideline 同時明確指出 patient advocate 作為 panel 正式成員的角色(p.845-846)。
Driving Force Classification
Primary driver: Expert consensus shift + Multiple viable options now available
SDM 的形式化反映了一個根本性的臨床現實改變:2025 年的 DTC management 存在多個同樣 viable 的選項(AS vs surgery vs ablation for PTMC;lobectomy vs TT for T2;RAI vs no RAI for low-risk)。當 evidence 支持多條合理路徑時,patient preference 成為 tiebreaker。這不是「證據不足所以讓患者選」,而是「證據顯示多條路徑同樣安全,所以讓患者的價值觀引導選擇」。
Secondary drivers:
- Patient advocate on panel
- Implementation feedback from 2015 guideline era
- Healthcare quality movement (value-based care, patient-centered outcomes)
12. De-escalation Narrative Analysis(去強化敘事分析)
12.1 是否存在連貫的 de-escalation 哲學?
是的。 2025 guideline 展現了一個明確的、跨領域的 de-escalation cascade:
更多 lobectomy (R15)
-> 更少 completion thyroidectomy (R16)
-> 更少 prophylactic CND (R19)
-> 更少 RAI (R32)
-> 更少 TSH suppression (R45-46)
-> 更短/可終止的 surveillance (R48)
-> "Complete remission" 終點
這些變化不是孤立的 -- 它們形成了一個相互強化的系統。例如:lobectomy 的擴大使得 RAI(需要 TT 作為前提)自然減少;RAI 的省略使得 TSH suppression 的論點減弱;surveillance 的去強化則是上述所有改變的下游邏輯結果。
12.2 De-escalation 是否有足夠的證據支持?
De-escalation 證據最強的領域
- RAI omission in low-risk:兩項 Phase III RCTs(Level 1 evidence)
- rhTSH preferred over withdrawal:7 項 RCTs 的 meta-analysis
De-escalation 證據中等的領域
- Lobectomy expansion:多項 registry studies 一致但均為 retrospective
- pCND against:多項 meta-analyses 一致但均基於 retrospective studies
De-escalation 證據最弱的領域
- Active surveillance:無 RCT;依賴單一機構 30 年回顧性數據
- Complete remission / surveillance stopping:主要為 expert consensus + limited retrospective data
- TSH suppression relaxation:no RCT comparing TSH targets
結論
De-escalation narrative 的總體方向是合理且有支持的,但其證據基礎不均勻。在 RAI decision 上有最強的 RCT 支持;在 surgery extent 和 pCND 上有大量但品質次等的 registry data 支持;在 surveillance de-escalation 上則主要依賴 expert consensus。
12.3 複合效應:病患旅程的轉型性改變
Compounding effect 值得特別關注:對於一個典型的 1.5 cm cT1bN0M0 PTC 患者:
| 決策點 | 2015 年路徑 | 2025 年路徑 |
|---|---|---|
| 手術 | Equipoise → 多數接受 total thyroidectomy | Lobectomy(Strong recommendation,≤2 cm) |
| 預防性 CND | 經常執行 | Strong 推薦不做(cT1/T2 cN0) |
| RAI | 多數 DTC 患者均被考慮 | Strong/High 反對(低風險 DTC) |
| 甲狀腺荷爾蒙 | 終身 L-T4 | 70–80% 的 lobectomy 患者完全不需要 |
| TSH 目標 | 依初始風險的靜態目標 | 依 DRS 的動態目標;excellent response → 正常範圍 |
| 監測 | 無限期 Tg + US | 有時限:US 5–8 年後可停(TT 路徑);10–15 年 complete remission |
⚠️ 警示: 每一步的 de-escalation 都有其獨立的 evidence support。ESTIMABL2 和 IoN Trial 的患者均接受 total thyroidectomy。每個單獨組件各有循證依據,但整合路徑的長期安全性尚無直接前瞻性資料。所有步驟同時 de-escalate 的 combined safety 的組合路徑(lobectomy + 無 RAI + TSH 正常 + 降低監測)從未在前瞻性研究中作為 combined pathway 被驗證。這是 2025 guideline 最重要的 evidence gap。